

To understand the FAA’s current policy governing the licensing of pilots, one must understand the history involved.
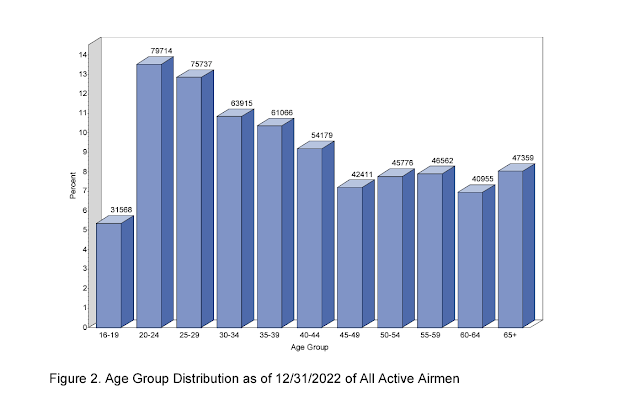
First, I think it is fair to say that piloting and the business of flying have been and are strongly influenced by the military. Many commercial pilots were trained in the military, and historically, policy has been informed by standards that exist there. As a result, both the civilian and military have similar organizational structures. While the FAA provides top-down policy to the Aviation Medical Examiner (AME), the military dictates policy to the air unit’s flight surgeon. Both groups of clinicians have clear fitness guidelines that must be met and maintained before pilots are allowed to fly.However, it can be argued that civilian AME have a harder task. They are asked to evaluate and sign-off on older pilots than those typically seen in the military. It is no secret that as we age, we accumulate all sorts of things – some good, some bad. And these brushes with life can often lead to physical or mental health issues. The following graph illustrates the age breakdown of all FAA certified pilots on 12/31/22 (source: 2022 Aerospace Medical Certification Statistical Handbook).
Additionally, military pilots are mandated to keep in good physical shape – they are expected to regularly exercise. They are frequently timed and tested to ensure that they are, indeed, exercising. In contrast, nobody is or can force civilian pilots to remain in shape. Or, that is, until obesity is diagnosed by the AME. So, in general, one might expect military pilots to be younger, more fit, and by far, healthier.

The military also has the advantage of being a one-source repository of information. If a pilot gets ill, the military manages their care and has full access to the medical records. So, a flight surgeon can look up an airman’s medical info and does not need to rely on the pilot’s self-admission. Contrast that with the AME – they have no such database. They need to rely on what they can see, measure, or are told.
So, summarizing: both systems take a top-down and regulation-based approach towards clearing pilots. One – the military – has a healthier population and an excellent bank of data regarding the pilot. The other, the FAA, has an older and more challenging population to clear. And, they do so with imperfect data. Here is a graph illustrating that – as pilots age, there are more of them needing special licenses that accommodate their medical issues.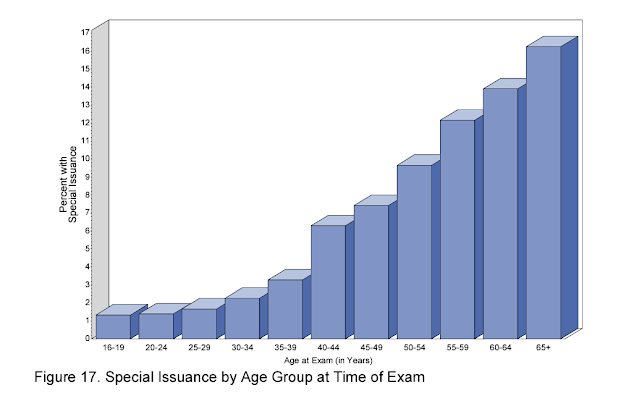
As a result, the FAA compensates by (1) demanding full disclosure from pilots and (2) asking for exhaustive testing when a possible issue is uncovered. As they don’t have all the info, the FAA is forced to look for pilots that are minimizing or outright lying.
Consequently, the role of the AME becomes adversarial. The FAA and the AME’s don’t particularly like to see the situation in this light and minimize it. They claim to be an ally of pilots and ask for their trust. But, in truth, seeing an AME is sort of like having an IRS audit. Everyone in the room is pleasant and they might even try to like each other but, make no mistake about it, it is a dangerous conversation that can devastate one’s career.
Informally and off-the-record, many AMEs express some level of discomfort with their dual role as doctors and police. And, indeed, the FAA is aware of that. Here is an extended passage from the FAA’s online “Guide for Aviation Medical Examiners: Application Process for Medical Certification: General Information - Legal Responsibilities of Designated Aviation Medical Examiners”
The consequences of a negligent or wrongful certification, which would permit an unqualified person to take the controls of an aircraft, can be serious for the public, for the Government, and for the Examiner. If the examination is cursory and the Examiner fails to find a disqualifying defect that should have been discovered in the course of a thorough and careful examination, a safety hazard may be created and the Examiner may bear the responsibility for the results of such action.
Of equal concern is the situation in which an Examiner deliberately fails to report a disqualifying condition either observed in the course of the examination or otherwise known to exist. In this situation, both the applicant and the Examiner in completing the application and medical report form, may be found to have committed a violation of Federal criminal law which provides that:
"Whoever in any matter within the jurisdiction of any department or agency of the United States knowingly and willfully falsifies, conceals, or covers up by any trick, scheme, or device a material fact, or who makes any false, fictitious or fraudulent statements or representations, or entry, may be fined up to $250,000 or imprisoned not more than 5 years, or both" (Title 18 U.S. Code. Secs. 1001; 3571).
Cases of falsification may be subject to criminal prosecution by the Department of Justice. This is true whether the false statement is made by the applicant, the Examiner, or both. In view of the pressures sometimes placed on Examiners by their regular patients to ignore a disqualifying physical defect that the physician knows to exist, it is important that all Examiners be aware of possible consequences of such conduct.
Be certain -- noncompliance by the AME carries with it serious risk.
So, let’s assume the AME identifies a medical issue. Then, the train starts moving. And nothing, absolutely nothing, has the weight and mass to stop that engine from chugging away.
And there, it sits. For months. But, again, I am getting ahead of myself. More on that later but, for now, back to mental health issues.
At that point, the AME just becomes a shepherd – they collect the specialists’ notes, determine if the content is adequate, and walk through the FAA checklist. Is everything there? Is it properly signed and dated? Does it address the specific demands of the FAA? If so, they package it all together and forward it to the FAA.
The French Mountain
What if, as is true with most cases of depression, the medical issue is not readily visible or measurable? How does the FAA make the pilots disclose all their issues? Never mind that pilots tend to be stoic, as a culture. The cockpit work environment is all about maintaining control and squelching emotion – “the Right Stuff”. So talking about depression – or even recognizing one’s own depression – might be a big leap. But it’s a giant, enormous, monumental, Evel-Knievel-over-the-grand-canyon leap if disclosure means losing one’s job for, as we shall see, perhaps two years or longer. Why would someone volunteer such information?
Many pilots may disclose because it is “the right thing to do.” But, for the others, the same hammer the FAA wields over the AMEs also threatens the pilot. And, it is a very frightening hammer. It is a felony to lie or mislead the AME. If you do so you can lose your piloting license. But, in addition, one can be fined up to $250,000 and/or be sent to jail for up to 5 years.
We will return to this “hammer” in a future blog entry but, first, let’s discuss a few more historical events – sentinel events – that have influenced the FAA.
Since 1982, there have been at least 6 incidents where it is widely believed a mentally ill pilot intentionally crashed an aircraft and killed passengers. There are many more deaths that just involved pilots alone in a plane but let’s limit this discussion to murder-suicides. Briefly:
- 2/9/82: Japan Air Lines Flight 350. Japan. Pilot tried to crash the jet during landing. He and the flight crew wrestled in the cockpit before the plane dropped short of the runway. There were 24 fatalities but he and 149 others survived. The Captain was later found to have paranoid schizophrenia and the lack of adequate medical exams was blamed.
- 8/21/94. Royal Air Maroc Flight 630. Morocco. Pilot dived into the ground after disconnecting the autopilot. The First Officer tried to intervene. The pilot had been cleared in a routine medical exam some 4 weeks earlier. 44 fatalities.
- 12/19/97. Silk Air Flight 185: Sumatra. Pilot was having disciplinary problems and was deep in debt. It was also the anniversary date of several military colleagues’ deaths. The pilot is believed to have locked his copilot out of the cockpit. 104 fatalities.
- 10/31/99, Egypt Air Flight 990. Atlantic Ocean. The copilot appears to have put the plane into a dive. The pilot, who seems to have been out of the cockpit initially, returns and wrestles with the flight controls as the copilot seems to obstruct a recovery. The copilot is reported as having disciplinary issues with the airline and the person who had demoted him was a passenger. 217 fatalities.
- 11/29/13 LAM Mozambique Air Flight 470. Namibia. Again, the copilot was locked out of cockpit and the plane was crashed into the ground. The pilot had lost his son to suicide nearly to the day, one year earlier and the pilot’s daughter had just been hospitalized for a serious ailment. 33 fatalities.
- 3/24/15. Germanwings Flight 9525. France. Was flown into a French mountainside by its copilot. Again, the other flight crew member (the pilot) was locked out of the cockpit. The copilot had seen many physicians, had well-established recurrent depression, and falsely believed he was going blind. He was told he was unsafe to fly by his physician and, after his death, the doctor’s letter was found in the trash. Apparently, German law prevented the physician from alerting others. The copilot of Germanwings was previously denied a US pilot license due to his history of depression. 150 fatalities
Why are these murder-suicides important? Well, obviously, there are lessons to be learned. One lesson? Do not leave the flight deck with only one pilot and, if you must, ensure that the lock combo cannot be changed – an issue in nearly all the cases. But I believe this is already widely addressed in policy. Then, what else do I make of this (tragic) list?
Well, from the FAA’s perspective, they see murder-suicide as an ongoing risk. And, to mitigate that risk, pilots should not fly if they are depressed or have a history of recurrent depression. The Germanwings event was taken as evidence of that, as seen in the FAA’s report to Congress on July 12, 2023 (Report AV2023038). The FAA recommendations? A slow, plodding pace towards…more studies.
Now, from a psychiatrist’s perspective, I see the situation differently. First, there is a need for some urgency in a FAA change in policy. Pilots should have access to mental health providers with no repercussions, at all. Second, I argue that if the pilots above had been engaged in treatment, most of these events were preventable. Specifically:
- Psychosis is not hard to detect, especially if it presents in the illness schizophrenia (Japan Airlines).
- The Egypt Air, Silk Air, and Germanwings incidents all involved disciplinary and work conflict issues. If addressed in treatment, anger and homicidal thought very likely would have emerged. It is near impossible to hide the sort of rage needed to plan a mass murder and your own suicide.
- From what little detail we have, the LAM pilot was flying during a period of multiple clear, severe, and predictable stressors: a son’s death, a daughter’s illness, and a marriage’s dissolution. All topics likely to be discussed and considered in treatment.
- As for the psychosomatic and psychotic depression (Germanwings), it was detected. Unfortunately, German law manages confidentiality differently than in the United States and the pilot was not stopped from flying.
I am left with three questions:
Could these and other depressed pilots be engaged in treatment?
If the FAA permitted pilots to see therapists and psychiatrists and get FAA-approved care without suspending their license, there would be few incentives to avoid treatment. And by FAA-approved care, I mean treatments that are not likely to impair judgment, reaction time, cause seizures, hypoglycemia, etc while the pilot flies. The FAA already has a list of such medications.
This invitation to treatment without career repercussions could be counterbalanced by the FAA’s hammer: if the pilot is depressed and not seeking care but, instead, hiding from it, they should risk all the same things they already do today – i.e., licensure revocation, hefty fines, and felony charges. Putting it differently, if the pilot is so impaired that they are making unreasonable choices in avoiding treatment, they should also face the normal FAA enforcement tools.
If engaged in care, could tragic events like those listed above, be prevented?
I think so. Psychiatrists and mental health practitioners have an obligation to complete and total confidentiality, with very few exceptions. One of those special cases is called the Tarasoff warning; all 50-states have some variant of it. By and large, Tarasoff indicates that the law dictates that mental health providers have a special duty to protect others if there is a specific, imminent, and likely threat of harm.
The clearest example of the usefulness of a Tarasoff warning in the above incidents would be the Germanwings flight. There, the copilot was known to be dangerous – so much so that his German doctor wrote him a letter saying that. However, rather than accomplish anything, the letter probably further inflamed the pilot and likely fueled his anger and paranoia. The letter was counterproductive and dangerous. But, German law apparently did not permit a more useful warning.
In the USA, this incident would have led to a Tarasoff intervention. It could have taken many forms – most likely a mandated hospitalization to preserve the pilot’s confidentiality while still protecting the public. There, a medical team would then work on a safe discharge plan. Alternatively, if a hospitalization was not an option, a warning to the police and/or airline would have been reasonable.
Thus, if a guidebook for treating pilots could be developed – what are the permitted meds at what doses, what meds must be avoided, who to contact if Tarasoff is needed, emergency numbers to the airline and FAA, etc – the legal precedent and framework for protecting the public is already in place,
This solution would lead to fewer pilots being grounded for depression. Wouldn’t that mean, then, that more pilots were flying with depression? Would this make the skies riskier?
Well, I would argue that those same depressed pilots are flying, right now. As discussed in my last blog, very few pilots are admitting to depression – far too few to be anything but a vast undercount. So, the question should be rephrased. Which would you want in the cockpit: a pilot being monitored and treated for depression or a depressed pilot, hiding their illness?
Next blog installment: Bureaucratic Purgatory – a Deep Dive into FAA Deferrals




Interesting!
ReplyDelete