
Let’s dig deeper.
When a pilot sees an Aviation Medical Examiner (AME), there are three possible outcomes: They can get their renewal, they can be banned from flying planes, or their pilot license can be deferred.
A renewal is good for a certain amount of time. It differs according to your age and the classification of the pilot. Commercial pilots have more frequent renewals than, say, someone driving a piston aircraft. And older pilots have their medical clearances expire sooner than their younger colleagues.
But regardless of when the medical exam is due, all pilots are supposed to report to an AME if they develop a new health condition, no matter where they are on the AME timeclock. They usually don't, but policy is that they should.
In a September 2019 letter to the American College of Occupational and Environmental Medicine, a prior study of 325 pilots was discussed. Around 71% of pilots did not seek care when appropriate. The authors also discussed a second study of 151 aircrewman. There, 55% did not seek care when ill with upper respiratory symptoms.
The authors went on to survey 613 pilots and found that almost four of every five pilots were worried about their careers when seeking care. 60% of them reported delaying getting care and 39% withheld medical data when they did eventually see a doctor. Note this: with these 613 pilots, we are talking about them merely seeing a doctor. If they fear what the physician is going to document, you can imagine the reluctance they would have in dialing up an AME.

These findings are widely confirmed and have been for decades. In a 2002 study by Wiegmann, autopsies were reviewed on 559 pilots from 498 fatal aircraft accidents. The exams revealed 1% of the pilots had acute myocardial infarctions (MI) – heart attacks. But, nearly half of those that had MIs also had advanced arterial stenosis. One might fairly suppose that they were symptomatic with angina and other symptoms before the fatal event and they did not alert their AMEs of the symptom. If they had, they would have been grounded, pending the medical workup.
So, pilots are supposed to alert their AMEs of new medical issues between scheduled visits, but generally don't. Why? Because they fear the rejections and deferrals that AMEs trigger.

That said, very few pilots are outright rejected. Most AMEs issue a deferral and leave it to the FAA’s physicians to deal out the bad news. After all, the pilot can't fly on a deferral. And by giving a deferral, you avoid really pissing off the person sitting in front of you – someone you probably like.
A deferral, on the other hand, is much more common and not at all clearcut. With mental health issues, neither the pilot nor the AME can predict an outcome or time course.
This week, I asked my staff to call the FAA and ask “What is the average time it takes to process a deferral?” The response was "6 weeks." Honestly, I don’t know what to make of this. With regards to mental health, this is sheer rubbish. 9-months seems about the minimum. Industry lawyers and pilots going through the process push that out considerably. By all accounts, it is not unusual to see delays of a full year to year-and-a-half before the FAA processes a “deferral.” I have spoken to pilots at the 2- and 3-year marks and a lawyer who described clients working on 4-year deferrals.
Although the FAA tracks the delay, their data is not publicly available. It should be. As much as any other data point, the delay in processing deferrals is a clear index of how well the FAA is doing its job. Pilots don't trust the system or the FAA's ability to manage it. So, if basic questions like "How long will the deferral take?" are not answered, pilots are left reasonably skeptical. There is no transparency, no reality check, no accountability, and a huge risk to the pilots’ livelihood. Paranoia is the appropriate response.
Indeed, the FAA can answer the question. They know how long the deferral process takes. The data exists, they track it, and it is even obliquely referenced in their testimony and publications. But the FAA does not publish the data in the same way they meticulously report to the public the age or weight of pilots. They opt not to.
That, of course, strongly suggests the data is embarrassing to the agency. It is one thing for pilots to "know" from the grapevine that they might be on deferral for 500+ days for taking an antidepressant. But to read it in black-in-white might make people angry. It might make them call for change. And to have such an easily understood benchmark of the agency's performance in public view, year-to-year, might make some managers uncomfortable, especially if the trendline went badly.
Enter the ARC – the Mental Health & Aviation Medical Clearances Aviation Rulemaking Committee – and their April 1st, 2024 final report. ARC was a broad-based independent committee consisting of industry experts, clinicians, pilots, FAA staffers, and others. It was created to advise the FAA on addressing mental health challenges after the Germanwings murder-suicide air crash (see last blog).
Lo and behold, what the FAA has not published, the ARC did...a little bit. We will come back to this report in a future blog entry. I will say that the ARC report hit on many of the same observations that I continue to talk about, including this one:

"Trust requires open communication, shared expectations, transparency with a commitment to reliability, and credibility by all parties. Justified or not, pilots/controllers lack trust that the FAA will manage the medical certification application process fairly and in a timely manner...." (Mental Health & Aviation Medical Clearances, Aviation Rulemaking Committee, Recommendation Report, April 1, 2024)
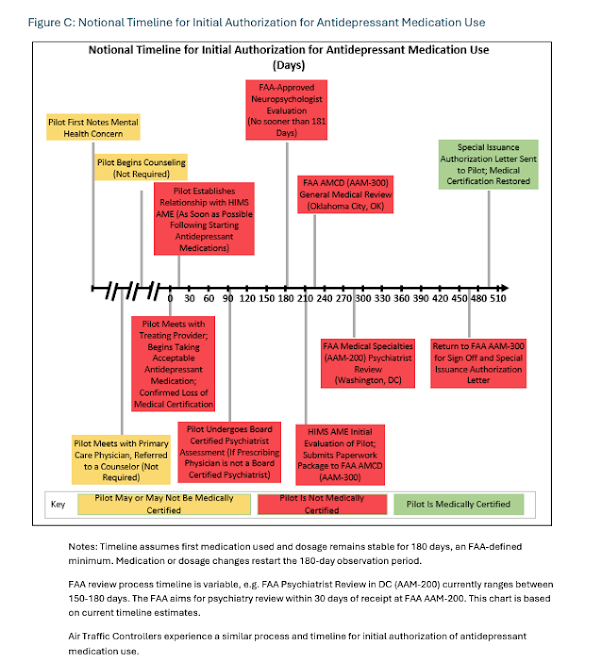
But, back to processing delays on deferrals. Here is a typical timeline that the ARC report documented, illustrating the processing of an antidepressant deferral. In this case, the turn-around time was shown to be around 500 days. So the reports of delays are not anecdotal – they are documented in the federal record.
The time delay of a deferral is determined by several components. First, there is the period between the submission of the deferral by the AME and the processing of it by the FAA. In the recent past, this involved US Mail and clerks. I don't know whether this has been fixed but here is what the ARC had to say about it in April of this year:
The ARC also notes the extremely slow pace of the process due to the FAA’s heavy reliance on the US Mail and limited ability to receive/submit documentation electronically. For professionals accustomed to making time critical decisions, waiting weeks to months for feedback is demoralizing and can adversely impact many mental health issues.
A little sidenote, if you will forgive me. Back in 2003, the FAA began a comprehensive effort to upgrade its processes and computer systems. Appropriately, they called it NextGen. The hope was to take the agency from one that relied on outdated technology from the 1950's and outfit it with modern tools and methods. It is estimated that by 2030, the final cost of the refit will exceed $30 billion.
However, the NextGen project has suffered epic mismanagement. Hundreds of millions have been redirected and zeroed out. Most goals are either very delayed or have been outright dropped from the plan. Those items that have been implemented are quite limited. What has not been limited, however, is the degree of grief the NextGen project has harnessed. The project has become the dependable punching bag for the FAA’s Office of the Inspector General, Congress, various presidents, the airlines, and pretty much everyone in between. The lack of modernization and the Agency's inability to adequately manage the expenditure of billions has been an ongoing embarrassment that also presents serious safety risks. And, it also explains why the FAA can't yet manage electronic documents and processes, such as medical reviews.
Anyways, after the mail is picked up, sorted, and filed, the FAA reviews the deferral. But therein lies another delay. The FAA can't recruit adequate numbers of medical providers. They are woefully understaffed and the wages they offer have been uncompetitive. (Note: I was told by a lawyer that the psychiatry wages at the FAA may have increased very recently; by all accounts, the FAA was paying about $100,000 below other comparable government psychiatry positions and was half-staffed relative to need.)
So, they are short-staffed. In talking with AMEs and lawyers that work with the FAA, they widely praise the staff that are there. Invariably, though, they also note that there are too few of them and the throughput is slow.
Interestingly, this problem is compounded by a large increase in AME deferrals. Pilots are aging. And yes, aging pilots will develop more health issues and require more deferrals. (Incidentally, commercial pilots must retire at age 65.)
But here is the "interesting" part: Many more young pilots are being flagged by the AMEs.
Why are young pilots getting dinged? Well, as a society, there has been an explosion in the diagnosis of ADHD and depression. And, in many cases, the Gen Z pilots were given stimulants or psychiatric diagnoses when they were younger. Thus, they are flagged by the AME.
So there are delays in the deferral system due to processing issues at the FAA, staff shortages, and the increased number of deferrals. These same issues take a toll with each step that involves the FAA. But there is another large source for the delay and this issue is not under the FAA's control. It rests on the pilots.
After the deferral is logged and reviewed, the FAA will require certain exams before the case is resolved. The pilot will be required to hire a variety of experts and have them produce extensive reports. It is formulaic. If someone had pneumonia, the expectation might be a respiratory consult and clinical letter to the FAA. Perhaps the FAA might also require chest imaging or an MRI. I believe the FAA has standard protocols for most medical disorders.
In the case of depression, the FAA will request that the pilot see a board-certified psychiatrist and later, get neuropsych testing. Finding and scheduling such appointments leads to more delays. Moreover, it is hard to book appointments with the expert specialists – those with the byzantine knowledge of pilot care.
The pilot needs an aviation expert psychiatrist because there are landmines to be avoided – normal words and medications and diagnoses that, if documented, will turn the FAA’s apparatus into a blood frenzy that will wildly delay any licensure. General psychiatrists don’t have a clue about this.
The normal standards and treatment algorithms do NOT apply to the treatment of pilots. A prescriber is often forced to settle for substandard treatments or have the pilot face a permanent job loss. And the typical psychiatrist will not expect or like the frequent voluminous reports required by the FAA. So getting into care with someone knowledgeable and proficient who does not screw up your appeal can take months.
Then there is stabilization. The FAA requires at least 6 months of no medication changes and stable mood before considering a reinstatement of the license. In addition, there are numerous reports that must say the right things – and not just from the psychiatrist. You need them from the initial AME, from an airline supervisor/peer, from the neuropsychologist, and from the HIMS (Human Intervention Motivational Study) AME.
The visits and documentation continue until the health concern either goes away, is stabilized, or the pilot gives up on trying to reverse the deferral. In the meantime, the costs of the medical exams and workup are all covered by the pilot.
This amounts to something like purgatory. The pilot is paying a bundle of money to satisfy the FAA while, at the same time, is unable to work. Disability might help and cover, say, 60-80% of base salary but that sounds better than it is. A pilot might be paid their base for 75 hours of flight time a month. But many will push that to, perhaps, 90 hours. There is, after all, a shortage of pilots and helping out your airline with some extra hours is both a good thing to do and also lucrative. So, if a pilot was hired for, say, $100,000 base, they might be doing an extra 15 hours and making another $40,000, for a total of $140,000. On disability, they are given $60,000 and have a new boatload of medical charges. Less money and more expenses over a long period with no predictable outcome…purgatory.
But it is often worse. Different pilot unions have different disability packages. One commercial carrier, for example, will pay disability for one year. As we have seen, many FAA deferrals easily exceed that. Some go for two or three years, or longer.
Next blog I hope to discuss the specific FAA requirements and criteria for permitting pilots with depression. We will explore the normal pathway and the "Fast Track." Theoretically, the Fast Track is preferred and a recent innovation of the FAA. But, if we are being honest, without the pilot actively lying or the AME overlooking a boatload of information, the odds of being sent to the Fast Track is about as likely an outcome as tripping into a pile of rancid dinosaur dung on some jungle island. Hey, it happens… in the movies. Until then, please send me your comments and/or corrections.




No comments:
Post a Comment